
microbiology round
2024年8月15日のMicrobiology Roundは、Clostridium perfringensを取り上げました。
ポイントは下記です。
・Clostridium属は環境中に存在し、土壌汚染を伴う外傷後の感染症で起炎菌になる。
・Clostridium属は種によってグラム染色の見え方が異なり、グラム陰性菌に見えるものもある。
・Clostridium perfringensの殆どはペニシリンに感受性があり、ペニシリンで治療が可能である。
【歴史】(1)
・”klôstêr”:a spindle(紡錘)→”Clostridium”:a small spindle。”perfringens”:breaking through(突破)、breaking in pieces(粉砕)
・C. perfringensは1891年、William H. Welchによって38歳の男性の剖検から初めて分離され、新種の細菌として同定された。このガス形成特性(原名は「Bacillus aerogenes capsulatus」で、'aerogenes'はラテン語で'空気を産生する'という意味)は、後に第一次世界大戦中にイギリスとフランスの兵士に見られたガス壊疽の症状と関連していた(2)
・Clostridium属には300を超える種が記載されている。
【微生物学】(3,4)
・Clostridium属は、土壌や水などの自然環境に広く存在しており、ヒトや虫、動物の腸管内に存在する。
・Clostridium属は基本的に偏性嫌気性菌だが、C. tertium、C. histolyticum、C. innocuum、C. perfringensのような少数のClostridium属は耐気性(aerotolerant)があり、Bacillus属と誤認されることがある(3)。
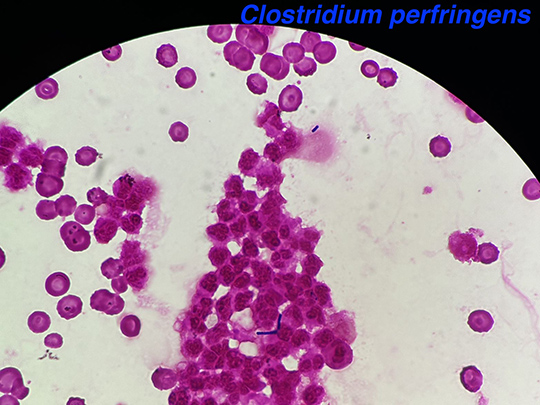
・Clostridium属は基本的にグラム陽性に染色されるが、C. clostridioforme や C. ramosum、C. innocumやC. hathewayiなどの種は、典型的なグラム陽性桿菌のような外観を示すことは殆どなく、gram-variableまたはgram-negative rodsに見える(3)。多形であり、短い鎖状、クラスター状、あるいは対になっている。殆どの種で末端は丸い。芽胞を形成する位置は菌種によって異なり、C. perfringensは中心または中心〜端である。
・多くのClostridium属はカタラーゼ試験陰性だが、C. perfringensなどの一部では陽性になることがある。cytochrome systemを持たないので、オキシダーゼ試験は陰性(4)。
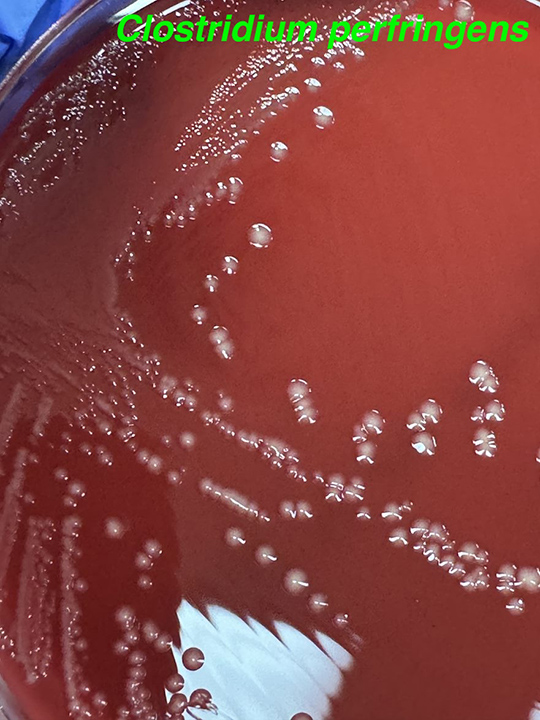
・コロニーは黄色〜灰色で不透明、直径4〜8mm、境界は不規則で、内側のβ溶血帯を外側の部分溶血帯が取り囲む特徴的な二重溶血帯を示す。α-toxin (レシチナーゼ)は、トリグリセリドを豊富に含む卵黄寒天培地上での増殖によって検出できる。コロニーを取り囲む明らかな白色沈殿は、レシチナーゼ産生の証拠である。特異的抗血清によるこの反応の中和(Nagler反応)は、C. perfringensの同定の推定的な証拠となる。α-toxin (レシチナーゼ)は細胞膜に損傷を与えるため、重症敗血症では急激な溶血性貧血をきたすことがある。殆どのC. perfringensの株は、ヘモリシン、プロテアーゼ、コラゲナーゼ、ヒアルロニダーゼ、デオキシリボヌクレアーゼやノイラミニダーゼも産生する(5–7)。
・嫌気性菌が血液培養から検出されることは約0.5〜6%と少ないが、血液培養から分離される嫌気性菌の中ではClostridium属がBacteroides属に次いで多く、全体の約12〜24%と報告されている(8–11)。別の報告では、Clostridium属の菌血症138例のうち、C. perfringensが最も多く(58例/42%)、次いでC. septicum (19例/14%)であった(12)。
・Clostridium属の菌血症のリスク因子には、血液透析、悪性腫瘍、Crohn病、心疾患や糖尿病などが報告されている(12)。ある研究では、C. septicumが血液培養で検出された患者の24.2%が、大腸癌を合併していたと報告されている(13)。
【臨床所見】(3)
・C. perfringens感染症の病型は、侵襲性感染症(主に皮膚軟部組織感染症)とenterotoxinによる食中毒がある。
■Clostridial Myonecrosis (Gas Gangrene:ガス壊疽)
・ガス壊疽は主に外傷性(traumatic)と、非外傷性(spontaneous)に大別される。
・外傷性のガス壊疽は、C. perfringensによる汚染外傷によるものが最多である。素因となる条件としては、細菌芽胞を含む土壌に汚染された、圧挫症や大・中サイズの動脈の裂傷、長骨の開放骨折などがある。腹壁のガス壊疽は、ナイフや銃創のような貫通性の損傷で腸管が破綻し、腸内容物が軟部組織に漏出した後に起こる(14)。ガス壊疽は、アメリカ南北戦争、第一次世界大戦、第二次世界大戦において、傷の治療が遅れたためによく見られた(4)。C. perfringensやC. novyi type A、C. sordelliiによる皮膚のガス壊疽は、米国や北欧において、「ブラック・タール・ヘロイン(精製不十分で不純物が残っていることにより、タールのように粘着性があり、石炭のように黒く硬いヘロイン)」を皮下注射する薬物乱用者の間で報告されている(15–17)。
・外傷性のガス壊疽は、外傷から24〜72時間(平均は24時間未満)後に、突然の激しい疼痛や腫脹で発症する。出血性水疱が、"mousy"と表現される漿血性分泌物や特徴的な臭気とともに生じることがある。臭気は、グラム陰性嫌気性菌感染に伴う揮発性アミンの産生による腐敗臭とは異なる。α-toxinが好中球を高度に破壊するため、グラム染色では好中球は認められないことも多い(18)。血管内の血小板凝集とフィブリン沈着による微小血管循環の閉塞が、重篤な虚血につながる(19)ため、(炎症により血流を増加する)多くの軟部組織感染症とは異なり、ガス壊疽に起因する病変は容易に出血しない(20)。C. perfringensのθ-toxinであるperfringolysin Oも、α-toxinと相乗的に作用して微小血管の灌流を低下させる可能性がある。
・目の貫通性外傷や角膜移植によるC. perfringensの眼内炎も報告されている(21–23)。
・非外傷性のガス壊疽は、主に消化管の入口から細菌(多くはC. septicum)が筋肉に血行性に播種されることによって起こる(14)。感染部位は急速に疼痛や腫脹が出現し、透明、白濁、出血性、または紫色を帯びた液体の水疱が見られる(24,25)。消化管病変は、一般的に結腸癌であり、他のリスク因子としては憩室炎、消化管や筋骨格系移植片手術、白血病、リンパ増殖性疾患、抗癌化学療法・放射線療法やacquired immunodeficiency syndrome (AIDS)が報告されている(14,26)。C. septicumのα-toxinは、C. perfringensとは異なりホスホリパーゼC活性を持たず、明確な機序は不明である(27)。
■腹腔内感染症、胆道感染症(3)
・腸管内容物による汚染から生じる腹腔内感染は、多くの場合は複数菌感染で、Clostridium属は他の偏性嫌気性菌や通性菌とともに膿瘍からしばしば分離される。B. fragilisや腸内細菌科などの微生物は感染における病原性が確立されているが、Clostridium属の腹腔内感染症における病原性は明らかではない。
・C. perfringensによる腹壁の壊死性感染症は、C. perfringens単一菌によるものと考えられている。
・Clostridium属は、胆道系感染症の20%以上から分離される。胆道感染症で分離されるClostridium属の50%を、C. perfringensが占める。一部の症例では、胆嚢内腔にガスが存在することがある。
■女性の生殖器感染症(3)
・Clostridium属は、正常な膣微生物叢の一部として女性の約10%の生殖管から分離される。
・頻度は少ないが、C. perfringensやC. sordelliiによる産後や中絶後の感染症は重症化する可能性がある(28,29)。胎児や胎盤組織への感染により、羊膜絨毛膜炎として発症する。子宮壁や子宮内膜組織に広がる可能性がある。
・子宮のガス壊疽(特にC. sordelliiによるもの)は、歴史的には違法な流産や自己誘発流産の結果として起こってきたが、現代では自然流産、正常経膣分娩、帝王切開の後にも起こる(30)。C. sordelliiはまた、医学的に誘発された中絶にも関与している(31)。分娩後の致死的なC. sordellii感染症に罹患した、それまで健康であった若い女性は、発熱が殆どないか、膿性分泌物がなく、難治性の低血圧、広範な末梢の浮腫と胸水、血液濃縮、白血球数の著明な上昇という独特な臨床像を呈する(31)。これらの症例では急速に死に至り、致死的である(4)。
■食中毒(Food Poisoning)(3)
・Clostridium属による食中毒のうち、C. perfringens type Aがほぼ全ての原因である。
・適切な調理や保存がなされていない汚染食品が摂取されると、小腸内で胞子形成し、enterotoxinを放出する。このenterotoxinは、哺乳類の細胞に損傷を与えるという点で、細胞毒素であると考えられる。
・潜伏期間は7~15時間(範囲は6〜24時間)で、症例は24~48時間以内に自然治癒する。
【治療】
・ヒトから検出されたC. perfringensの殆どが、ペニシリン、カルバペネム、メトロニダゾールなどにin vitroで感受性が良好である(32–34)。クリンダマイシンも多くは感受性があるが、耐性の報告もある(J Tissue Viability. 2008 Aug;17(3):95-7)(Anaerobe. 2014 Aug:28:120-5)。一方で、ヒト以外の動物から検出された株では、ペニシリン耐性率が約10〜20%との報告もある(35,36)。
・クリンダマイシンやテトラサイクリンは、ペニシリンよりも速やかにα-toxinの合成を阻害する(37)。
・ガス壊疽の場合には、迅速な感染組織の除去(débridement)が最も重要である(3)。高圧酸素療法は十分なデータがなく有効性は不明であり(38)、Infectious Diseases Society of America (IDSA)のガイドラインでも殆どの場合に推奨していない(39)。
【参考文献】
1. LPSN - List of Prokaryotic names with Standing in Nomenclature “Clostridium perfrigens” [Internet]. [cited 2024 Aug 27]. Available from: https://lpsn.dsmz.de/species/clostridium-perfringens
2. Welch WH& NGHF. A gas-producing bacillus (Bacillus aerogenes capsulatus, Nov, Spec.) capable of rapid development in the body after death. Bull John Hopkins Hosp Baltim. 1891;3:81–91.
3. Andrew B. Onderdonk and Wendy S. Garrett. 246 Diseases Caused by Clostridium. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 2020. p. 2960-2968.e2.
4. Ed J. Kuijper FAGR and FB. 56 Clostridium, Clostridioides, and Other Clostridia. In: Karen C. Carroll and Michael A. Pfaller, editor. Manual of Clinical Microbiology. 13th ed. 2023.
5. Kiu R, Hall LJ. An update on the human and animal enteric pathogen Clostridium perfringens. Emerg Microbes Infect. 2018 Dec 6;7(1):1–15.
6. Camargo A, Ramírez JD, Kiu R, Hall LJ, Muñoz M. Unveiling the pathogenic mechanisms of Clostridium perfringens toxins and virulence factors. Emerg Microbes Infect. 2024 Dec 31;13(1).
7. Rood JI, Adams V, Lacey J, Lyras D, McClane BA, Melville SB, et al. Expansion of the Clostridium perfringens toxin-based typing scheme. Anaerobe. 2018 Oct;53:5–10.
8. Robert R, DeRaignac A, Moal G, Ragot S, Grollier G. Prognostic factors and impact of antibiotherapy in 117 cases of anaerobic bacteraemia. European Journal of Clinical Microbiology & Infectious Diseases. 2008 Aug 21;27(8):671–8.
9. Dumont Y, Bonzon L, Michon AL, Carriere C, Didelot MN, Laurens C, et al. Epidemiology and microbiological features of anaerobic bacteremia in two French University hospitals. Anaerobe. 2020 Aug;64:102207.
10. Zouggari Y, Lelubre C, Lali SE, Cherifi S. Epidemiology and outcome of anaerobic bacteremia in a tertiary hospital. Eur J Intern Med. 2022 Nov;105:63–8.
11. Kovács K, Nyul A, Lutz Z, Mestyán G, Gajdács M, Urbán E, et al. Incidence and Clinical Characteristics of Anaerobic Bacteremia at a University Hospital in Hungary: A 5-Year Retrospective Observational Study. Antibiotics. 2022 Sep 28;11(10):1326.
12. Leal J, Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species bacteremia in Calgary, Canada, 2000–2006. Journal of Infection. 2008 Sep;57(3):198–203.
13. Justesen US, Ellebæk MB, Qvist N, Iachina M, Frimodt-Møller N, Søes LM, et al. Colorectal cancer and association with anaerobic bacteraemia: A Danish nationwide population-based cohort study. Journal of Infection. 2024 Aug;89(2):106212.
14. Stevens DL, Aldape MJ, Bryant AE. Life-threatening clostridial infections. Anaerobe. 2012 Apr;18(2):254–9.
15. Centers for Disease Control and Prevention (CDC). Update: Clostridium novyi and unexplained illness among injecting-drug users--Scotland, Ireland, and England, April-June 2000. MMWR Morb Mortal Wkly Rep. 2000 Jun 23;49(24):543–5.
16. Bangsberg DR, Rosen JI, Aragón T, Campbell A, Weir L, Perdreau-Remington F. Clostridial Myonecrosis Cluster Among Injection Drug Users. Arch Intern Med. 2002 Mar 11;162(5):517.
17. Kimura AC, Higa JI, Levin RM, Simpson G, Vargas Y, Vugia DJ. Outbreak of Necrotizing Fasciitis Due to Clostridium sordellii among Black-Tar Heroin Users. Clinical Infectious Diseases. 2004 May 1;38(9):e87–91.
18. O’Brien DK, Therit BH, Woodman ME, Melville SB. The role of neutrophils and monocytic cells in controlling the initiation of Clostridium perfringens gas gangrene. FEMS Immunol Med Microbiol. 2007 Jun;50(1):86–93.
19. Bryant AE, Chen RYZ, Nagata Y, Wang Y, Lee CH, Finegold S, et al. Clostridial Gas Gangrene. II. Phospholipase C–Induced Activation of Platelet gpIIbIIIa Mediates Vascular Occlusion and Myonecrosis in Clostridium perfringens Gas Gangrene. J Infect Dis. 2000 Sep;182(3):808–15.
20. Hickey MJ, Kwan RYQ, Awad MM, Kennedy CL, Young LF, Hall P, et al. Molecular and Cellular Basis of Microvascular Perfusion Deficits Induced by Clostridium perfringens and Clostridium septicum. PLoS Pathog. 2008 Apr 11;4(4):e1000045.
21. Hsu HY, Lee SF, Hartstein ME, Harocopos GJ. Clostridium perfringens Keratitis Leading to Blinding Panophthalmitis. Cornea. 2008 Dec;27(10):1200–3.
22. Guedira G, Taright N, Blin H, Fattoum T, Leroy J, El Samad Y, et al. Clostridium perfringens panophthalmitis and orbital cellulitis: a case report. BMC Ophthalmol. 2018 Dec 10;18(1):88.
23. Centers for Disease Control and Prevention (CDC). Clostridial endophthalmitis after cornea transplantation--Florida, 2003. MMWR Morb Mortal Wkly Rep. 2003 Dec 5;52(48):1176–9.
24. Stevens DL, Musher DM, Watson DA, Eddy H, Hamill RJ, Gyorkey F, et al. Spontaneous, Nontraumatic Gangrene Due to Clostridium septicum. Clinical Infectious Diseases. 1990 Mar 1;12(2):286–96.
25. Johnson S, Driks MR, Tweten RK, Ballard J, Stevens DL, Anderson DJ, et al. Clinical Courses of Seven Survivors of Clostridium septicum Infection and Their Immunologic Responses to Toxin. Clinical Infectious Diseases. 1994 Oct 1;19(4):761–4.
26. Kainer MA, Linden J V., Whaley DN, Holmes HT, Jarvis WR, Jernigan DB, et al. Clostridium Infections Associated with Musculoskeletal-Tissue Allografts. New England Journal of Medicine. 2004 Jun 17;350(25):2564–71.
27. Ballard J, Bryant A, Stevens D, Tweten RK. Purification and characterization of the lethal toxin (alpha-toxin) of Clostridium septicum. Infect Immun. 1992 Mar;60(3):784–90.
28. McGregor JA, Soper DE, Lovell G, Todd JK. Maternal deaths associated with Clostridium sordellii infection. Am J Obstet Gynecol. 1989 Oct;161(4):987–95.
29. Snow M. On alert for postpartum C. sordellii infection. Nursing (Brux). 2008 Jan;38(1):10.
30. Aronoff DM, Marrazzo JM. Infections caused by Clostridium perfringens and Paeniclostridium sordellii after unsafe abortion. Lancet Infect Dis. 2023 Feb;23(2):e48–55.
31. Aldape MJ, Bryant AE, Stevens DL. Clostridium sordellii Infection: Epidemiology, Clinical Findings, and Current Perspectives on Diagnosis and Treatment. Clinical Infectious Diseases. 2006 Dec 1;43(11):1436–46.
32. Roberts SA, Shore KP, Paviour SD, Holland D, Morris AJ. Antimicrobial susceptibility of anaerobic bacteria in New Zealand: 1999–2003. Journal of Antimicrobial Chemotherapy. 2006 May 1;57(5):992–8.
33. Wybo I, Van den Bossche D, Soetens O, Vekens E, Vandoorslaer K, Claeys G, et al. Fourth Belgian multicentre survey of antibiotic susceptibility of anaerobic bacteria. Journal of Antimicrobial Chemotherapy. 2014 Jan;69(1):155–61.
34. Brook I, Wexler HM, Goldstein EJC. Antianaerobic Antimicrobials: Spectrum and Susceptibility Testing. Clin Microbiol Rev. 2013 Jul;26(3):526–46.
35. Wu D, Luo R, Gong G, Zhang L, Huang J, Cai C, et al. Antimicrobial susceptibility and multilocus sequence typing of Clostridium perfringens isolated from yaks in Qinghai-Tibet plateau, China. Front Vet Sci. 2022 Oct 17;9.
36. Khademi F, Sahebkar A. The prevalence of antibiotic-resistant Clostridium species in Iran: a meta-analysis. Pathog Glob Health. 2019 Feb 17;113(2):58–66.
37. Stevens DL, Maier KA, Mitten JE. Effect of antibiotics on toxin production and viability of Clostridium perfringens. Antimicrob Agents Chemother. 1987 Feb;31(2):213–8.
38. Kaide CG, Khandelwal S. Hyperbaric Oxygen: Applications in Infectious Disease. Emerg Med Clin North Am. 2008 May;26(2):571–95.
39. Stevens DL, Bisno AL, Chambers HF, Dellinger EP, Goldstein EJC, Gorbach SL, et al. Executive Summary: Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2014 Jul 15;59(2):147–59.
このサイトの監修者
 亀田総合病院
亀田総合病院
臨床検査科部長、感染症内科部長、地域感染症疫学・予防センター長 細川 直登
【専門分野】
総合内科:内科全般、感染症全般、熱のでる病気、微生物が原因になっておこる病気
感染症内科:微生物が原因となっておこる病気 渡航医学
臨床検査科:臨床検査学、臨床検査室のマネジメント
研修医教育
