
microbiology round
2024年8月8日のMicrobiology Roundでは、Aerococcus spp.を取り上げました。
ポイントは下記3点です。
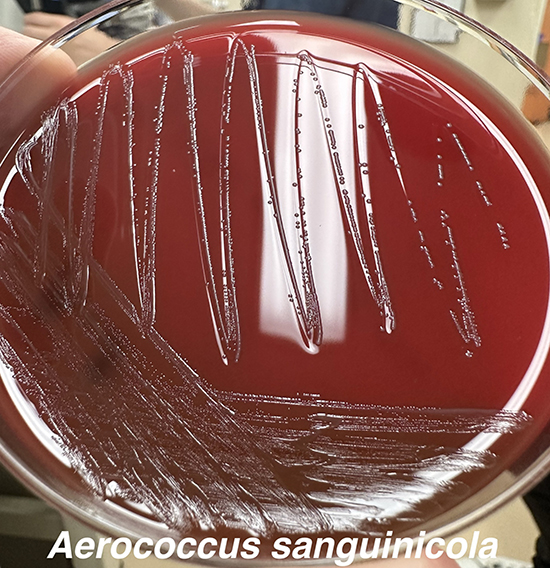
・グラム染色ではGPC cluster、血液寒天培地上のコロニーはS. viridans様。
・基礎疾患がある患者の尿路感染症が多いが、感染性心内膜炎の報告も多数ある。
・ペニシリン系抗菌薬の感受性が良いことが多く、多くの症例で使用されている。
【歴史】(1)
・”aer”:「air、gas」、”coccus”:「a berry (球菌)」、”sanguis”:「blood」、”-cola”:「dweller (住人、居住者)」、”urinae”:「of urine (尿の)」。
・1953年に居住区の粉塵・空気中で発見され、最初はAerococcus viridansと名付けられた(2)。その後、1967年以降に徐々にヒト感染症の起因菌として報告されるようになり、1992年にA. urinae (3)、2001年にA. sanguicola (後にA. sanguinicolaに変更)が報告された(4)。
・他のAerococcus属は、A. vaginalis (膣から)、A. urinaehominis (尿から)など、合計13種類が報告されている(1)。
【微生物学的特徴】(5)
・Aerococcus属は、グラム染色で約1~2µmのグラム陽性球菌の不規則な集塊として観察される(2)。
・オキシダーゼ試験とカタラーゼ試験は陰性。A. sanguinicolaはpyrrolidonyl arylamidase production (PYR)、leucine aminopeptidase production (LAP)、β-glucuronidase activity (BGUR)の全てが陽性。一方で、A. urinaeはそのうちPYRのみ陰性で、A. viridansはLAPのみ陰性。
・通性嫌気性菌だが、A. viridansは嫌気条件下では殆ど発育しない(5)。A. viridansはα溶血性コロニーを形成し、staphylococciやstreptococci、enterococciと歴史的には誤同定されることが多かった(6)。生化学的検査では、特にA. sanguinicolaはA. viridansとして、A. urinaeはGranulicatellaとして誤同定される可能性が高い(7)。matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS)や16S rRNA gene sequencingによるA. urinaeやA. sanguinicola、A. viridansの同定の精度は高い(8,9)。
・A. urinae、A. sanguinicolaは、尿路感染症を起こすことが多い(10)。また、尿路感染症を契機とする敗血症や感染性心内膜炎を引き起こすことが報告されている(11)。2菌種とも、バイオフィルム形成と血小板凝集という2つのメカニズムで病原性を発揮していると考えられている(12,13)。
・A. urinaeは、血液や尿培養で他の菌と同時に検出されることも多々ある(14)。
【臨床的特徴】
・尿路感染症:Aerococciは尿培養から0.2〜0.8%の頻度で分離され、そのうちA. urinaeが55〜66%、A. sanguinicolaが26〜46%を占め、A. viridansは稀である(6)。高齢男性や、背景に前立腺肥大症や前立腺癌、尿路結石・閉塞などの泌尿器疾患、または膀胱カテーテル留置があることが多い(14)。尿路感染の症状や細菌尿があるにもかかわらず、培養でAerococcus属が検出されないことが多いが、Aerococcus属がCO2を含む環境でないと培養されにくいことが原因の可能性がある(6)。
・感染性心内膜炎:Aerococcus属による感染性心内膜炎の症例報告は多く(11,15)、A. urinaeによるものが最も多い(6)。現状、A. sanguinicolaによる感染性心内膜炎の報告はA. viridansよりも少ないが、これは誤同定による可能性が指摘されている(16)。A. urinaeによる感染性心内膜炎の死亡率は約27%と報告されている(15,17)が、2016年のスウェーデンからの16例の症例集積研究では、死亡例は0例であったとの報告もある(18)。塞栓症の合併や手術が必要な割合は、α溶血性連鎖球菌や腸球菌による感染性心内膜炎に近い(18)。
・他の感染巣:Aerococcus属による侵襲性感染症の多くは菌血症で、原因は尿路感染症が多い(6)。稀な感染巣としてはCAPD腹膜炎、椎体炎、外陰部皮膚軟部組織感染、産褥感染、歯性感染、関節炎、手術部位感染症などの報告がある(6)。
【治療】
■抗菌薬感受性
・2016年のThe Clinical and Laboratory Standards Institute (CLSI)におけるA. sanguinicolaとA. urinae、A. viridansに対する抗菌薬のブレイクポイント(CLSI M45 ED3:2016)では、ペニシリンとセフォタキシム、セフトリアキソン、メロペネム、バンコマイシン、シプロフロキサシンとレボフロキサシン、テトラサイクリン、スルファメトキサゾール・トリメトプリム、リネゾリドが設定されている(19)。一方、The European Committee on Antimicrobial Susceptibility Testing (EUCAST)では2017年にA. sanguinicolaとA. urinaeにのみブレイクポイントが設定され、2024年1月1日のEUCASTで設定されている抗菌薬は、ベンジルペニシリン、アンピシリン、アモキシシリン、メロペネム、シプロフロキサシン、レボフロキサシン、ノルフロキサシン、バンコマイシン、ニトロフラントイン、リファンピシンのみである(20)。
・A. sanguinicolaとA. urinaeに対する、ペニシリンやアンピシリンの抗菌薬感受性は100%に近い(6,11,14)。セフトリアキソンはminimal inhibitory concentration (MIC)がやや高い傾向にあるが、感受性があることが多い(14)。A. viridansに対するブレイクポイントは設定されていないが、MICはA. sanguinicolaとA. urinaeよりも高い傾向にある(11)。
■治療選択
・A. sanguinicolaとA. urinaeによる尿路感染症や菌血症に対する第一選択薬は定まっていないが、基本的にはペニシリンGやアンピシリンが使用され、βラクタムが使用できない場合にはバンコマイシンが使用されている(6)。
・A. urinaeによる感染性心内膜炎に対する第一選択薬も定まっていない。βラクタム系抗菌薬に加えて、in vitroの研究(21,22)を元にシナジー効果を目的としたアミノグリコシドが併用されていることが多い(15)が、その後の大規模な研究では、シナジー効果は少数の分離株でしか証明できなかったと報告されている(18)。
・A. urinaeはスルファメトキサゾールに内因性耐性があり、スルファメトキサゾール・トリメトプリムに対する感受性結果は培地に依存する。特にウマ血液を含む培地は感受性を示し、他のいくつかの場合には耐性を示す(6)。また、MICはEテストと微量液体希釈法で結果が異なることがある(23)。
・フルオロキノロン系抗菌薬のMICは、特にA. sanguinicolaでは比較的高く(24)、一般的に耐性であり(23)、gyrA遺伝子またはparC遺伝子の変異を介している(25)。
1. LPSN - List of Prokaryotic names with Standing in Nomenclature “Aerococcus” [Internet]. [cited 2024 Aug 13]. Available from: https://lpsn.dsmz.de/genus/aerococcus
2. Williams REO, Hirch A, Cowan ST. Aerococcus, a New Bacterial Genus. J Gen Microbiol. 1953 Jun 1;8(3):475–80.
3. Aguirre M, Collins MD. Phylogenetic analysis of some Aerococcus-like organisms from urinary tract infections: description of Aerococcus urinae sp. nov. J Gen Microbiol. 1992 Feb 1;138(2):401–5.
4. Lawson PA, Falsen E, Truberg-Jensen K, Collins MD. Aerococcus sanguicola sp. nov., isolated from a human clinical source. Int J Syst Evol Microbiol. 2001 Mar 1;51(2):475–9.
5. Xiaohui Chen Nielsen and JJC. Aerococcus, Abiotrophia, and Other Aerobic Catalase‐Negative, Gram‐Positive Cocci. In: Karen C. Carroll and Michael A. Pfaller, editor. Manual of Clinical Microbiology. 13th ed. 2023.
6. Rasmussen M. Aerococcus : an increasingly acknowledged human pathogen. Clinical Microbiology and Infection. 2016 Jan;22(1):22–7.
7. Cattoir V, Kobal A, Legrand P. Aerococcus urinae and Aerococcus sanguinicola, two frequently misidentified uropathogens. Scand J Infect Dis. 2010 Oct 20;42(10):775–80.
8. Senneby E, Nilson B, Petersson AC, Rasmussen M. Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry Is a Sensitive and Specific Method for Identification of Aerococci. J Clin Microbiol. 2013 Apr;51(4):1303–4.
9. Derya Carkaci XCN. 16S-23S Intergenic Spacer (ITS) Region Sequence Analysis: Applicability and Usefulness in Identifying Genera and Species Resembling Non- Hemolytic Streptococci. Clinical Microbiology: Open Access. 2013;
10. Shelton-Dodge K, Vetter EA, Kohner PC, Nyre LM, Patel R. Clinical significance and antimicrobial susceptibilities of Aerococcus sanguinicola and Aerococcus urinae. Diagn Microbiol Infect Dis. 2011 Aug;70(4):448–51.
11. Tai DBG, Go JR, Fida M, Saleh OA. Management and treatment of Aerococcus bacteremia and endocarditis. International Journal of Infectious Diseases. 2021 Jan;102:584–9.
12. Shannon O, Mörgelin M, Rasmussen M. Platelet Activation and Biofilm Formation by Aerococcus urinae , an Endocarditis-Causing Pathogen. Infect Immun. 2010 Oct;78(10):4268–75.
13. Senneby E, Eriksson B, Fagerholm E, Rasmussen M. Bacteremia with Aerococcus sanguinicola: Case Series with Characterization of Virulence Properties. Open Forum Infect Dis. 2014 Mar 1;1(1).
14. Sihvonen R, Turunen M, Lehtola L, Pakarinen L, Grönroos JO, Rantakokko-Jalava K, et al. Clinical and microbiological characterization of Aerococcus urinae bacteraemias at Helsinki metropolitan area, Finland. European Journal of Clinical Microbiology & Infectious Diseases. 2022 May 8;41(5):751–60.
15. Saeed Al-Asad K, Mazhar N, Srivastava S, Quadri S, Mitra S. Aerococcus Urinae Endocarditis: A Case Report and Literature Review. Cureus. 2022 Oct 3;
16. Rasmussen M. Letter To The Editor. Canadian Journal of Infectious Diseases and Medical Microbiology. 2014 Jan;25(4):232–232.
17. Yabes JM, Perdikis S, Graham DB, Markelz A. A rare case of Aerococcus urinae infective endocarditis in an atypically young male: case report and review of the literature. BMC Infect Dis. 2018 Dec 17;18(1):522.
18. Sunnerhagen T, Nilson B, Olaison L, Rasmussen M. Clinical and microbiological features of infective endocarditis caused by aerococci. Infection. 2016 Apr 29;44(2):167–73.
19. Clinical and Laboratory Standards Institute. Methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated or fastidious bacteria. 3 rd ed. 2016; pp. M45-Ed3. 2016.
20. EUCAST, The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 14.0, valid from 2024-01-01 [Internet]. 2024 [cited 2024 Aug 13]. Available from: https://www.eucast.org/clinical_breakpoints
21. Skov R. In vitro antimicrobial susceptibility of Aerococcus urinae to 14 antibiotics, and time-kill curves for penicillin, gentamicin and vancomycin. Journal of Antimicrobial Chemotherapy. 2001 Nov 1;48(5):653–8.
22. Zbinden R, Santanam P, Hunziker L, Leuzinger B, von Graevenitz A. Endocarditis due toAerococcus urinae: Diagnostic tests, fatty acid composition and killing kinetics. Infection. 1999 Mar;27(2):122–4.
23. Senneby E, Petersson AC, Rasmussen M. Epidemiology and antibiotic susceptibility of aerococci in urinary cultures. Diagn Microbiol Infect Dis. 2015 Feb;81(2):149–51.
24. Facklam R, Lovgren M, Shewmaker PL, Tyrrell G. Phenotypic Description and Antimicrobial Susceptibilities of Aerococcus sanguinicola Isolates from Human Clinical Samples. J Clin Microbiol. 2003 Jun;41(6):2587–92.
25. Cattoir V, Kobal A, Legrand P. First Molecular Characterization of Fluoroquinolone Resistance in Aerococcus spp. Antimicrob Agents Chemother. 2011 Jan;55(1):451–2.

このサイトの監修者
 亀田総合病院
亀田総合病院
臨床検査科部長、感染症内科部長、地域感染症疫学・予防センター長 細川 直登
【専門分野】
総合内科:内科全般、感染症全般、熱のでる病気、微生物が原因になっておこる病気
感染症内科:微生物が原因となっておこる病気 渡航医学
臨床検査科:臨床検査学、臨床検査室のマネジメント
研修医教育
