
microbiology round
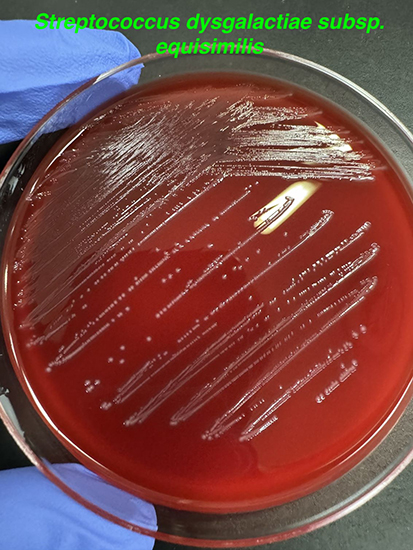
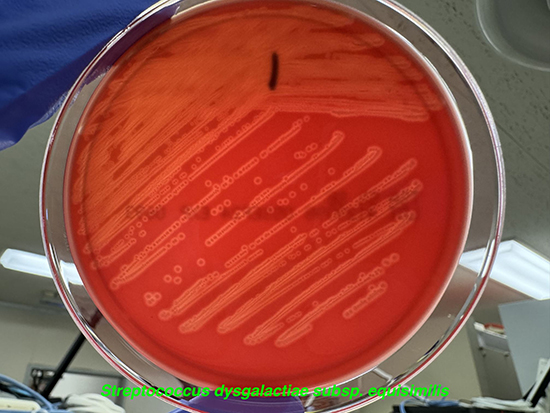
2024年7月4日のMicrobiology roundは、Streptococcus dysgalactiae subsp. equisimilisを取り上げました。
ポイントは下記です。
・SDSEは皮膚に定着していることが多く、上気道や消化管、女性生殖器にも常在する。
・SDSEの侵襲性感染症は、GASやGBSよりも高齢者に多く、背景に基礎疾患があることが多い。
・ペニシリン耐性のSDSEは非常に稀であり、ペニシリンが第一選択薬である。
【歴史・微生物学】(1)
・”streptos”=「pliant(曲がりやすい、柔軟な)」、”coccus”=「球菌」。” dys-“=「bad、hard(inseparable=不可分)の接頭詞」、”gala”=「milk」(→”dysgalactia”=「乳汁分泌の消失または低下」)。”equi”=「of a horse(馬の)」、”similis”= 「resembling(似ている)」。(2)
・S. dysgalactiae は、S. dysgalactiae subsp. equisimilis(SDSE)とS. dysgalactiae subsp. dysgalactiae (SDSD)に分類される(3)。SDSEは主にヒトの感染症から検出され、β溶血を示す。SDSDは主として動物由来であり、C群に属して溶血を示すものと示さないものが存在する。
・SDSEには、Lancefieldの分類のA、C、G、L群に分類される菌株が存在し、80%以上がG群、約15%がC群と報告されている(4)。
・SDSEは、バシトラシン試験感性、pyrrolidonyl arylamidase (PYR)試験陰性、Christie–Atkins–Munch-Peterson (CAMP)試験陰性、Voges-Proskauer (VP)試験陰性、馬尿酸加水分解陰性、トレハロース分解陽性、ソルビトール分解陰性(5)。
・Matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS)によるS. dysgalactiaeの同定は、他のStreptococcus属と比較してやや困難であった(6)が、データベースの改善に伴い同定率も向上してきている(7)。
・SDSEは皮膚に定着していることが多く、上気道や消化管、女性生殖器にも常在する(8)。
・SDSEの臨床所見はGASと似ている(8)。病原因子もGASと類似しおり、M蛋白(emm遺伝子によりコードされる)、ストレプトリジンO、ストレプトリジンS、ストレプトキナーゼA(ska)、ヒアルロニダーゼ(hyl)やStreptococcal C5aペプチダーゼ(scpA)、フィブロネクチン結合蛋白(fbp)、コラーゲン結合蛋白やラミニン結合蛋白(lmb)などの病原因子がある(9)。
■連鎖球菌とLancefield分類に関して
・Lancefieldの分類は Streptococcus属の細胞壁の多糖体の抗原の特異性から免疫学的に群別する方法(10)で、A~W(I、Jを除く)の群に分類される(11)。S. pneumoniaeとViridans streptococciは多糖体の抗原を持たず、”non-Lancefield streptococci”に分類される。
・まずは集落の大きさで識別され、S. pyogenes (GAS)とSDSEは大きいコロニー(24時間培養後の集落が0.5mm以上)、S. anginosus groupは小さいコロニー(0.5 mm未満)である(1)。B群はS. agalactiae (GBS)のみで、C群は先のSDSEとSDSDの他にS. equiとS. anginosus groupが含まれる。D群にはenterococciの一部とS. bovis group、F群にはS. anginosus group、G群にはSDSEのほかS. canis、S. anginosus groupが、L群にはSDSEも含まれる。RとS、T群にはS. suisが含まれる。
【臨床症状】
・SDSEの侵襲性感染症は、GASやGBSよりも高齢者(特に65歳以上)に多く、SDSE(やGBS)はGASよりも基礎疾患(糖尿病や悪性腫瘍、肝機能障害など)があることが多い(12,13)。
・主に皮膚に定着していることから、皮膚軟部組織感染症を起こすことが多い。明らかな感染巣のない菌血症(primary bacteremia)も多く、米国の212例のSDSE感染症の報告(4)では、感染巣は蜂窩織炎が41%、primary bacteremiaが26%、骨髄炎が9%、壊死性軟部組織感染症を含むStreptococcal toxic shock syndrome (STSS)が9%、化膿性関節炎が6%、感染性心内膜炎が3%であった。日本からのSDSE感染症の報告でも、感染巣は蜂窩織炎やprimary bacteremiaが多く、次いで壊死性軟部組織感染症や化膿性関節炎、椎体炎が多い(12,13)。
・SDSEは上気道に定着するため、急性咽頭炎を引き起こすことがあり、アウトブレイクの報告もある(14,15)。
・GASと同様に、急性糸球体腎炎や急性リウマチ熱の報告もある(16,17)。
・侵襲性SDSE感染症の死亡率は、約3~15%と報告されている(4,9,12,13)。
■S. pyogenes (GAS)感染症とSDSE感染症の比較(12,13)
①年齢:GAS感染症は学童、30歳代から増加して60歳代をピークに以後減少するが、SDSEは40〜50歳代を境に増加し、特に60歳以上に多い傾向がある。
②臨床所見:GASはprimary bacteremiaや局所の化膿性疾患、蜂窩織炎、壊死性筋膜炎、STSSが主な臨床所見である。SDSEは上記疾患に加えて、化膿性関節炎が多くみられる。
③基礎疾患:GAS感染症は約40%が明らかな基礎疾患がない患者で、SDSE感染症は約79%が何らかのリスクを有していたと報告されている(12)。
【治療】
・SDSEは、in vitroでも、β-ラクタム系抗菌薬(ペニシリン Gやアンピシリン、第1〜3世代セファロスポリン、メロペネム)やバンコマイシンに対して感受性がある(4,9)。ペニシリン耐性のSDSEの報告もある(18)が、極めて稀である。
・エリスロマイシンやクリンダマイシン、テトラサイクリンに対する耐性株が増加している(13)。マクロライド耐性率は、地域によって異なる(19,20)。erm(A)やerm(B)、mef(A)などが関与している(21)。日本の報告では、エリスロマイシンに対して 31.5%、ミノサイクリンに対して 30.8%、クリンダマイシンに対して25.5%であった(13)。
・フルオロキノロンに対する耐性率は低いが、parCやgyrAの変異によるレボフロキサシン耐性が報告されている(22)。
1. Karen C. Carroll and Michael A. Pfaller. 22 Streptococcus. In: Manual of Clinical Microbiology. 13th ed. 2023. p. 429–48.
2. LPSN - List of Prokaryotic names with Standing in Nomenclature “Subspecies Streptococcus dysgalactiae subsp. equisimilis” [Internet]. [cited 2024 Jul 12]. Available from: https://lpsn.dsmz.de/subspecies/streptococcus-dysgalactiae-equisimilis
3. Vandamme P, Pot B, Falsen E, Kersters K, Devriese LA. Taxonomic study of lancefield streptococcal groups C, G, and L (Streptococcus dysgalactiae) and proposal of S. dysgalactiae subsp. equisimilis subsp. nov. Int J Syst Bacteriol. 1996 Jul;46(3):774–81.
4. Broyles LN, Van Beneden C, Beall B, Facklam R, Shewmaker PL, Malpiedi P, et al. Population-based study of invasive disease due to beta-hemolytic streptococci of groups other than A and B. Clin Infect Dis. 2009 Mar 15;48(6):706–12.
5. Facklam R. What happened to the streptococci: overview of taxonomic and nomenclature changes. Clin Microbiol Rev. 2002 Oct;15(4):613–30.
6. Fan WT, Qin TT, Bi RR, Kang HQ, Ma P, Gu B. Performance of the matrix-assisted laser desorption ionization time-of-flight mass spectrometry system for rapid identification of streptococci: a review. Eur J Clin Microbiol Infect Dis. 2017 Jun;36(6):1005–12.
7. Nybakken EJ, Oppegaard O, Gilhuus M, Jensen CS, Mylvaganam H. Identification of Streptococcus dysgalactiae using matrix-assisted laser desorption/ionization-time of flight mass spectrometry; refining the database for improved identification. Diagn Microbiol Infect Dis. 2021 Jan;99(1):115207.
8. Brandt CM, Spellerberg B. Human infections due to Streptococcus dysgalactiae subspecies equisimilis. Clin Infect Dis. 2009 Sep 1;49(5):766–72.
9. Takahashi T, Ubukata K, Watanabe H. Invasive infection caused by Streptococcus dysgalactiae subsp. equisimilis: characteristics of strains and clinical features. J Infect Chemother. 2011 Feb;17(1):1–10.
10. Lancefield RC. A SEROLOGICAL DIFFERENTIATION OF HUMAN AND OTHER GROUPS OF HEMOLYTIC STREPTOCOCCI. J Exp Med. 1933 Mar 31;57(4):571–95.
11. Public Health England. UK Standards for Microbiology Investigations. 2022. “ID 4: Identification of Streptococcus species, Enterococcus species and morphologically similar organisms.”
12. Takahashi T, Sunaoshi K, Sunakawa K, Fujishima S, Watanabe H, Ubukata K, et al. Clinical aspects of invasive infections with Streptococcus dysgalactiae ssp. equisimilis in Japan: differences with respect to Streptococcus pyogenes and Streptococcus agalactiae infections. Clin Microbiol Infect. 2010 Aug;16(8):1097–103.
13. Shinohara K, Murase K, Tsuchido Y, Noguchi T, Yukawa S, Yamamoto M, et al. Clonal Expansion of Multidrug-Resistant Streptococcus dysgalactiae Subspecies equisimilis Causing Bacteremia, Japan, 2005-2021. Emerg Infect Dis. 2023 Mar;29(3):528–39.
14. Turner JC, Hayden FG, Lobo MC, Ramirez CE, Murren D. Epidemiologic evidence for Lancefield group C beta-hemolytic streptococci as a cause of exudative pharyngitis in college students. J Clin Microbiol. 1997 Jan;35(1):1–4.
15. Yamaguchi T, Kawahara R, Katsukawa C, Kanki M, Harada T, Yonogi S, et al. Foodborne Outbreak of Group G Streptococcal Pharyngitis in a School Dormitory in Osaka, Japan. J Clin Microbiol. 2018 May;56(5).
16. Hule GP, Karmarkar MG, Cameron A, Hase N, Khopkar U, Mehta PR, et al. Seropositivity for Antibodies to DRS-G, a Virulence Factor from Streptococcus dysgalactiae subsp. equisimilis, Is an Independent Risk Factor for Poststreptococcus Glomerulonephritis and Chronic Kidney Disease in Mumbai, India. Clin Vaccine Immunol. 2015 Aug;22(8):938–42.
17. Haidan A, Talay SR, Rohde M, Sriprakash KS, Currie BJ, Chhatwal GS. Pharyngeal carriage of group C and group G streptococci and acute rheumatic fever in an Aboriginal population. Lancet. 2000 Sep 30;356(9236):1167–9.
18. Fuursted K, Stegger M, Hoffmann S, Lambertsen L, Andersen PS, Deleuran M, et al. Description and characterization of a penicillin-resistant Streptococcus dysgalactiae subsp. equisimilis clone isolated from blood in three epidemiologically linked patients. J Antimicrob Chemother. 2016 Dec;71(12):3376–80.
19. Ip M, Lyon DJ, Leung T, Cheng AFB. Macrolide resistance and distribution of erm and mef genes among beta-haemolytic streptococci in Hong Kong. Eur J Clin Microbiol Infect Dis. 2002 Mar;21(3):238–40.
20. Brown DFJ, Hope R, Livermore DM, Brick G, Broughton K, George RC, et al. Non-susceptibility trends among enterococci and non-pneumococcal streptococci from bacteraemias in the UK and Ireland, 2001-06. J Antimicrob Chemother. 2008 Nov;62 Suppl 2:ii75-85.
21. Sunaoshi K, Murayama SY, Adachi K, Yagoshi M, Okuzumi K, Chiba N, et al. Molecular emm genotyping and antibiotic susceptibility of Streptococcus dysgalactiae subsp. equisimilis isolated from invasive and non-invasive infections. J Med Microbiol. 2010 Jan;59(Pt 1):82–8.
22. Biedenbach DJ, Toleman MA, Walsh TR, Jones RN. Characterization of fluoroquinolone-resistant beta-hemolytic Streptococcus spp. isolated in North America and Europe including the first report of fluoroquinolone-resistant Streptococcus dysgalactiae subspecies equisimilis: report from the SENTRY Antimicrobial Surveillance Program (1997-2004). Diagn Microbiol Infect Dis. 2006 Jun;55(2):119–27.
このサイトの監修者
 亀田総合病院
亀田総合病院
臨床検査科部長、感染症内科部長、地域感染症疫学・予防センター長 細川 直登
【専門分野】
総合内科:内科全般、感染症全般、熱のでる病気、微生物が原因になっておこる病気
感染症内科:微生物が原因となっておこる病気 渡航医学
臨床検査科:臨床検査学、臨床検査室のマネジメント
研修医教育
