
microbiology round
2024年6月20日のMicrobiology roundは、Proteus vulgarisを取り上げました。
ポイントは下記です。
・ウレアーゼ産生能力が高く、結石性腎盂腎炎の起因菌となることが多い。
・Proteus mirabilisと異なり、アミノペニシリン、第1世代と第2世代セファロスポリン(セフォキシチンを除く)に自然耐性である。
【歴史】
・“Proteus”…詩人ホメーロスの「オデュッセイア」で登場する、ポセイドンの群れの世話をし、無限に変身する能力を持つ“海の老人”である「Proteus」に由来する(1)。“vulgaris”…「usual、common」。
・Proteus属は、1885年Gustav Hauserが最初に記述し(2)、現在はP. mirabilis、P. vulgaris、P. penneri、P. hauseri、P. cibarius、P. terrae、P. hauseriの6種類と3つの未命名のもの(genomospecies 4、5、6)があり、80種類のO抗原血清型がある(3)。
【微生物学的特徴】(4)
・ProteusやProvidencia、Morganellaは、乳糖分解能がなく、フェニルアラニンデアミナーゼ(phenylalanine deaminase)を産生し、運動性がある腸内細菌科(Enterobacteriaceae)の通性嫌気性グラム陰性桿菌の一種。
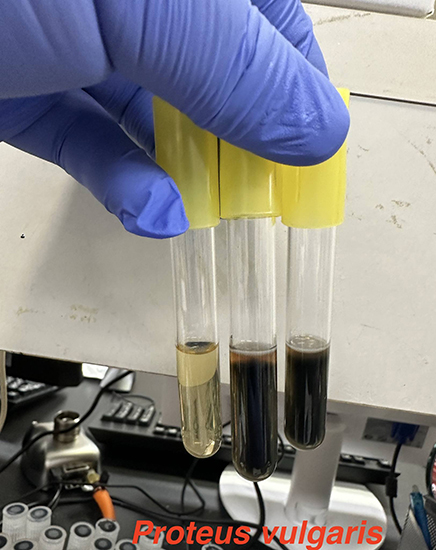
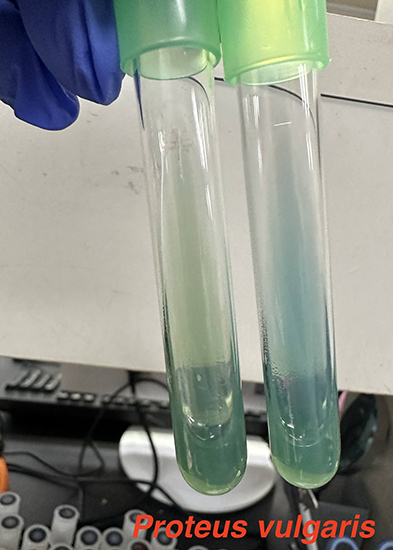
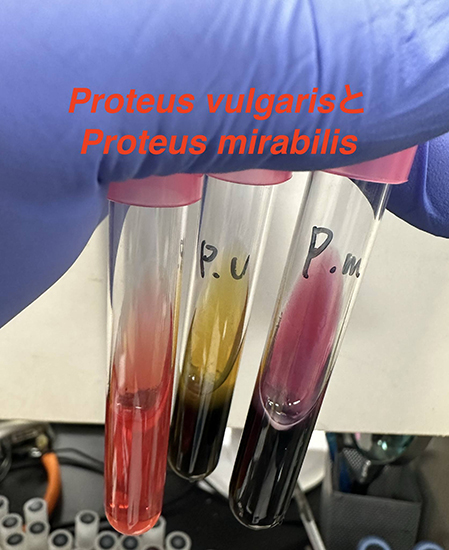
・Proteus mirabilisは臨床的に分離されるProteus属の90%を占めており、P. vulgarisと合わせて臨床的に分離されるProteus属の殆どを占めている。両方ともウレアーゼと硫化水素を産生し、P. mirabilisとP. hauseriはインドールピルビン酸(indole pyruvic acid :IPA)反応陰性で、P. vulgarisとP. penneriはIPA反応陽性である(5)。また、P. vulgarisのornithine decarboxylation (ODC) testは陰性だが、P. mirabilisは陽性である(3,5)。また、P. vulgarisはP. mirabilisよりもゼラチンの液化が速く、実験室での同定において鑑別に使用できる(6)。
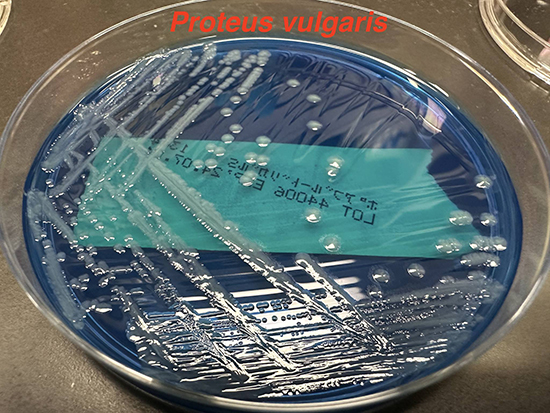
・Proteus属は多数の線毛と鞭毛を発現し、液体内では少ない鞭毛で「swimming」を起こして移動するが、寒天培地の表面では形を変えて「swarming」と呼ばれる特徴的な発育がある(7)。
・P. vulgarisは乾燥した硬い表面でも最大2日間残留するため、院内感染症の原因になる(8)。
・消化管内に保菌することがあり、野生または飼育されている様々な動物(哺乳類、爬虫類、鳥類、魚類など)からも分離されている(9)。
【臨床的特徴】(4,10)
・Proteus属は、腸内細菌目細菌による尿路感染症の中でE. coli やKlebsiellaに次いで多く、特に膀胱留置カテーテルや尿路の解剖学的・機能的異常がある患者で多い傾向にある。特にP. mirabilisによるカテーテル関連尿路感染症(catheter-associated urinary tract infections:CAUTI)では、マンノース耐性プロテウス様(mannose-resistant Proteus-like: MR/P)絨毛の発現が、初期付着とカテーテル上および膀胱内でのバイオフィルム形成に依存している。また、Proteus属はウレアーゼ産生能力が強く、ウレアーゼによって尿素を加水分解してCO 2とアンモニアを生成する。これにより尿がアルカリ化し、カルシウム結晶とリン酸マグネシウムアンモニウム沈殿物が生成され、これが多糖カプセルに取り込まれてカテーテル上に結晶性バイオフィルムを形成する(10)。特に尿pHが7以上の場合には、ウレアーゼ陽性菌(そのうち殆どがProteus属)による感染が示唆される。ウレアーゼ産生能は、P. vulgarisよりもP. mirabilisの方が高い(11)。Proreus属による尿路感染症の場合には、尿路結石やそれによる尿路閉塞の精査目的に、超音波検査やCT検査が考慮される(12)。
・他の感染巣としては、腹腔内感染症(消化管穿孔による二次性腹膜炎など)、熱傷や手術部位関連感染症、肺炎、膿胸、骨髄炎、新生児髄膜炎、脳膿瘍などの報告がある(3,6,13,14)。非P. mirabilis(特にP. vulgaris)では、尿よりも創部や皮膚軟部組織から分離される頻度が高い(15)。
【薬剤耐性と治療】(9)
・Proteus属は、ポリミキシン(コリスチン)、nitrofuran、チゲサイクリン、テトラサイクリンに内因性耐性がある(16)。ポリミキシンに対する耐性は、lipid Aの共有結合的修飾を介している(17)。
・P. mirabilisは染色体にコードされたβ-ラクタマーゼは存在しないため、野生型では全てのアミノペニシリンやセフェム系に感受性がある(6)。
・一方で、P. vulgarisは染色体にコードされた誘導性class A cefuroximase (Bush group 2e)を産生し(18)、アミノペニシリン、第1世代と第2世代セファロスポリン(セフォキシチンを除く)に耐性である。
・基質特異性拡張型βラクタマーゼ(Extended spectrum β-lactamases : ESBLs)やプラスミド誘導性AmpCβ-ラクタマーゼ、カルバペネマーゼなどのEnterobacteralesで報告されているほぼ全てのβ-ラクタマーゼが、Proteus属でも報告されている。P. mirabilisのESBLの最初の報告は1983年である(19)。
・Proteus属の野生株はフルオロキノロンに感受性があるが、キノロンの使用率が高い医療機関では耐性株が増えている。qnrやaac6’Ib遺伝子が関与している。アミノグリコシド耐性は、APHやAAC、AAD、methylases遺伝子が関与(9)。
【参考文献】
1. Wenner JJ, Rettger LF. A Systematic Study of the Proteus Group of Bacteria. J Bacteriol. 1919 Jul;4(4):331–53.
2. Hauser G. U¨ber fa¨ulnissbacterien und deren beziehungen zur septica¨mie. Ein betrag zur morphologie der spaltpilze. Vogel, Leipzig, Germany. 1885;
3. Drzewiecka D. Significance and Roles of Proteus spp. Bacteria in Natural Environments. Microb Ecol. 2016 Nov;72(4):741–58.
4. John E. Bennett MD R. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases [218 Enterobacteriaceae]. Ninth Edition. Vol. e13. 2020. 2669–2685 p.
5. Karen C. Carroll and Michael A. Pfaller. Manual of Clinical Microbiology. [41 Morganellaceae, Erwiniaceae, Hafniaceae, and Selected Enterobacterales]. In: 13th Edition. 2023. p. 817–25.
6. O’Hara CM, Brenner FW, Miller JM. Classification, identification, and clinical significance of Proteus, Providencia, and Morganella. Clin Microbiol Rev. 2000 Oct;13(4):534–46.
7. Schaffer JN, Pearson MM. Proteus mirabilis and Urinary Tract Infections. Microbiol Spectr. 2015 Oct;3(5).
8. Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006 Aug 16;6:130.
9. Girlich D, Bonnin RA, Dortet L, Naas T. Genetics of Acquired Antibiotic Resistance Genes in Proteus spp. Front Microbiol. 2020;11:256.
10. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015 May;13(5):269–84.
11. Jones BD, Mobley HL. Genetic and biochemical diversity of ureases of Proteus, Providencia, and Morganella species isolated from urinary tract infection. Infect Immun. 1987 Sep;55(9):2198–203.
12. Armbruster CE, Mobley HLT. Merging mythology and morphology: the multifaceted lifestyle of Proteus mirabilis. Nat Rev Microbiol. 2012 Nov;10(11):743–54.
13. Hau T. Bacteria, toxins, and the peritoneum. World J Surg. 1990;14(2):167–75.
14. Bloch J, Lemaire X, Legout L, Ferriby D, Yazdanpanah Y, Senneville E. Brain abscesses during Proteus vulgaris bacteremia. Neurol Sci. 2011 Aug;32(4):661–3.
15. Drzewiecka D, Palusiak A, Siwińska M, Zabłotni A. The prevailing O serogroups among the serologically differentiated clinical Proteus spp. strains in central Poland. Sci Rep. 2021 Sep 23;11(1):18982.
16. Stock I. Natural antibiotic susceptibility of Proteus spp., with special reference to P. mirabilis and P. penneri strains. J Chemother. 2003 Feb;15(1):12–26.
17. Olaitan AO, Morand S, Rolain JM. Mechanisms of polymyxin resistance: acquired and intrinsic resistance in bacteria. Front Microbiol. 2014;5:643.
18. Livermore DM. beta-Lactamases in laboratory and clinical resistance. Clin Microbiol Rev. 1995 Oct;8(4):557–84.
19. Knothe H, Shah P, Krcmery V, Antal M, Mitsuhashi S. Transferable resistance to cefotaxime, cefoxitin, cefamandole and cefuroxime in clinical isolates of Klebsiella pneumoniae and Serratia marcescens. Infection. 1983;11(6):315–7.

このサイトの監修者
 亀田総合病院
亀田総合病院
臨床検査科部長、感染症内科部長、地域感染症疫学・予防センター長 細川 直登
【専門分野】
総合内科:内科全般、感染症全般、熱のでる病気、微生物が原因になっておこる病気
感染症内科:微生物が原因となっておこる病気 渡航医学
臨床検査科:臨床検査学、臨床検査室のマネジメント
研修医教育
